Asian Review for Public Administration (ARPA)
Open Access | Research Article | First published online December 20, 2023
Vol. 31, Nos. 1&2 (January 2020 to December 2023)
Analyzing South Korea’s COVID-19 Policy Strategy Using a Regression Discontinuity Research Design
Gi Heon Kwon, Da Sol Lee, and Jungmin Hwang
Gi Heon Kwon, Da Sol Lee, and Jungmin Hwang
"Cite article"Kwon, G., Lee, D., & Hwang, J. (2020-2023). Analyzing South Korea’s COVID-19 Policy Strategy Using a Regression Discontinuity Research Design. Asian Review for Public Administration, Vol. 31, Nos. 1&2, 80-99. |
| ||
Abstract: Since its first outbreak in 2019, the coronavirus disease 2019 (COVID-19) pandemic has been one of the most devastating global disasters, resulting in millions of casualties worldwide. While governments have put tremendous efforts into controlling and eradicating the virus, the unprecedented nature of COVID-19 calls into question the government’s capacity for disease management. This study analyzed the effectiveness of South Korea’s COVID-19 policy by focusing on the causal relationship between instantaneous reproduction number, , and three different restriction policies: business closure, private gathering limit, and vaccine pass requirement. Using a sharp regression discontinuity design with a non-parametric estimation, this study found a positive effect of each restriction policy on decreasing . The results suggest that not only traditional restrictive strategies, such as business closure and gathering restriction, but also digital capacity could play a significant role in disaster management during global pandemics.
Keywords: COVID-19, Vaccine Pass, Regression Discontinuity Design, Reproduction Number, Disaster Management
Keywords: COVID-19, Vaccine Pass, Regression Discontinuity Design, Reproduction Number, Disaster Management
Introduction
An article on BBC (March 12, 2020) titled “Coronavirus in Korea: How 'trace, test, and treat' may be saving lives” stated, “as the coronavirus spreads rapidly around the world, killing thousands and leaving governments scrambling to deal with the fallout, one country has repeatedly drawn praise for its efficiency in dealing with it: South Korea.” Since the first confirmed case of COVID-19 was reported on 20 January 2020, South Korea has been coping with the virus using a wide range of policy measures. The Korea Disease Control and Prevention Agency (KDCA), which was the headquarters of disease management, started the production of diagnostic test kits after a massive-scale outbreak on 18 February 2020 in Daegu City. As fatality and infection numbers grew, social distancing became one of the major policy measures adopted to prevent the spread of COVID-19 (Kim 2021). With the introduction of a five-tier alert system, social distancing restricted large-scale gatherings and outdoor activities of the public. High-risk facilities for contracting the virus—such as restaurants, coffee shops, pubs, clubs, PC rooms, karaoke, and indoor event halls—had to be closed before 9 p.m., and even entirely shut down depending on the level of social distancing. In January 2021, the KDCA further issued a restriction on private gatherings of more than four people, which was the first and the most rigorous restriction.
Meanwhile, the South Korean government adopted a digital-data-based management to geolocate COVID-19 patients and trace people who had been closely in contact with them. For instance, when patients are identified, South Korean local governments sent them a real-time text message that provided self-quarantine rules, and placed them under self-quarantine for two weeks. The local governments also traced the places where the patients had visited, using the record of credit card transactions and the Global Positioning System (GPS) data of the patients’ mobile phones (Kim 2021). By sharing the traced information to the public through the “emergency-alert-system announcement,” the local governments were able to further identify close contacts of the patients. In more recent years, the South Korean government introduced a “vaccine pass” system which helped the identification of vaccinated citizens by using a quick response (QR) code. A person who had received more than two times of COVID-19 vaccination was allowed to patronize densely populated facilities.
In response to the government efforts for coping with the pandemic, a growing body of study has focused on comparing different types of COVID-19 policies and drawing the trend line of infection. However, most studies have been concerned with predicting future trends of infection rather than examining the policy effects against the spread of COVID-19 (Balmford et al., 2020; Hsaing et al., 2020; Pei and Shaman, 2020; Wibbens et al., 2020, Kim, 2021; Kim et al., 2021). In addition, only a few research examined the effectiveness of COVID-19 policies in South Korea (Lim, 2020; Lee and Hong, 2021; Nam and Lee, 2021). Given the various types of restriction policies that have been introduced within a short period of time, further research efforts examining the policy effects of COVID-19 countermeasures are required.
In this regard, this study examines the effectiveness of COVID-19 policies in South Korea. By focusing on social distancing rules, it reveals the causal relationship between COVID-19 policies and the reproduction number of the disease. Using a sharp regression discontinuity design with a non-parametric estimation, it focuses on three specific types of restrictions and examines each policy effect on restraining the virus transmission: (1) business closure, (2) private gathering limit, and (3) vaccine pass requirement. In this study, the weekly data of infectees and casualties from 17 metropolitan governments in South Korea are used. This study is expected to increase the understanding of COVID-19 policies in South Korea and add empirical evidence in disease disaster management.
Background of the Study
Government Response to Transmission Dynamics
The first case of COVID-19 in South Korea was reported on 20 January 2020—a Chinese national who had recently traveled from the province of Hubei, People’s Republic of China. On 18 February, the first massive COVID-19 outbreak in the country (as of November 2020) began with the 31st case of COVID-19 identified in Daegu, the fourth most populous metropolitan city of South Korea and home to 2.2 million individuals. Close contacts of the 31st case were particularly clustered around a nationwide religious group known as Shincheonji. By 8 March 2020, 4,482 positive cases were identified from the religious group, comprising the majority of the total of 7,478 cases. From then on, there was a quick decline in the number of domestic infections, meaning that imported cases once again comprised the majority. Apart from the Daegu outbreak in March, there were two notable domestic outbreaks: one occasion linked to an Itaewon nightclub in Seoul on 2 May and a considerably larger outbreak on 15 August, linked to political protests in Gwanghwamun, Seoul. Although these two outbreaks did not result in a surge of cases as sharp as the Daegu outbreak, these were notable events in terms of their impact on subsequent intervention rollouts and public controversies around privacy and compliance.
The government took interventions in quick response to the transmission dynamics. One of the first notable changes was the border policy. A mandatory quarantine period of 14 days had been in place since 1 April 2020. Another notable intervention featuring the government’s responsiveness is seen in its testing capacity for COVID-19, specifically the timeline for increasing the testing capacity. Two responsive interventions—border control and extensive testing—proved effective in mitigating the influx of exogenous cases of COVID-19 into the country. After following domestic outbreaks, central and local governments set new policies called social distancing on 29 February 2020. A more relaxed measure was implemented on 6 May 2020 when there was a decreased infection trend. Since then, the government changed the alert levels according to daily infection rates, which also implied that varying social distancing measures would take place accordingly.
In South Korea, COVID-19 is considered a serious public health emergency, and the situation is being managed as a national disaster response case, triggering the disaster response governance mechanism. According to the manual, the infectious disease response system operates on different alert levels. At Level 1, countermeasure teams are organized at the KDCA. The Central Disease Control Headquarters at the KDCA is formed and operated at Level 2, while the Central Disaster Management Headquarters is formed and supports the Central Disease Control Headquarters at Level 3. At the highest level (Level 4), the participation of the Central Disaster and Safety Countermeasure Headquarters (CDSCH) is activated.
The central role of the CDSCH is to undertake policy dialogues and decision-making for major policies such as social distancing, inter-ministerial coordination, and facilitation of discussion between central and local governments. The organizational structure is as follows. At the center of the structure is the head (currently the Prime Minister), while the deputy head is the Minister of Interior and Safety. Under the CDSCH’s supervision are the Central Disease Control Headquarters and Central Disaster Management Headquarters, the National Fire Agency, and the Coast Guard, which can directly dispatch and undertake response missions, as well as other ministries and agencies. Each of the ministries and agencies sometimes operates local units and organizations directly, or through working relationship channels with local government counterparts. As the CDSCH is a non-standing body, a COVID-19 operation center was established under the Prime Minister’s office to support the Prime Minister’s role as the CDSCH head. This COVID-19 operation center prepares CDSCH meetings, coordinates between ministries, and communicates directly with the Office of National Security or with the President. The COVID-19 operation center is within the Prime Minister’s office and is subdivided into teams: the general affairs team, which takes care of CDSCH meetings and risk communication; the supporting team, which provides daily operational support to the prime minister; and the current issue management team, which deals with current issues such as vaccine rollouts, and maintains relationships with medical communities.
Social Distancing Level
During the first wave in February 2020, South Korea had yet to implement a well-defined social distancing scheme. As the first wave peaked in March 2020, the government enhanced its social distancing measures in April and May 2020. When the number of confirmed cases stayed at the lowest level, the government refined the social distancing scheme for the first time and spelled out the plans according to each level. The scheme played a key role during the second wave. During the government’s response, there was a greater need for a more detailed plan. When the level retreated to Level 1 in October 2020, the government further refined the scheme and published the second amendment. In this revised policy, there were five levels of social distancing measures with specific details regarding the scope of each level. One of the key changes was that the local government was given the authority to set the social distancing level. Not long after the amendment, the third wave began at the end of November 2020. As situations in the metropolitan area and some regions aggravated, both the central and local governments reacted by increasing the social distancing level.
Regarding school closures, the government faced several difficult decisions. When the first wave broke out in February 2020, a new academic year was about to begin, but every school was kept closed until March 2020. The Ministry of Education directed schools to open virtually in April 2020, and as the first wave subsided, the Ministry of Education let the schools partially open. Gradually, students were able to go to schools under strict infection control measures, including hand washing, indoor and outdoor mask-wearing, physical distancing, daily check for symptoms, and self-isolation for those with symptoms. Consequently, South Korea did not face serious incidences of school-based infections.
Among the 127 confirmed adolescent cases from 1 May to 12 July 2020, only three were attributed to public education and kindergartens. Most cases were instead family (59 cases) and private lesson-related (18 cases) incidences. In the second semester, starting in late August 2020, more students were expected to attend school. However, only one-third to two-thirds of students were allowed to attend school at a time, when the exact number or percentage of students was dependent on the level of social distancing. Many academics and experts in the country stressed the importance of a continuum of education and policy measures to minimize education disparity and prevent domestic violence.
Restrictions on facilities with high infection risks were a crucial part of social distancing. All facilities were asked to maintain logbooks for visitors, check symptoms and temperatures at entrances, place hand sanitizers, deliver proper instructions to visitors, and disinfect venues regularly. Moreover, facilities such as restaurants, coffee shops, pubs, clubs, karaoke, and indoor concert and event halls were designated as facilities with a high risk of transmission. These facilities had to close before 9 p.m. or shut down entirely, depending on the level of social distancing. Some raised concerns over these restrictions, in particular the economic costs of social distancing that were not equally imposed and left the self-employed vulnerable. In December 2020, the country further issued a ban on private gatherings of more than four people, deeming it the highest level of restriction barring complete lockdowns.
Recently, Omicron has become a major variant, compared with Delta, which was much more contagious. The Korean government, responding to this new wave, updated its policy to impose social distancing and adopted a new monitoring system using self-diagnosis kits starting in February 2021. Although many medical experts optimistically predicted that the final stage of the COVID-19 pandemic was at hand, all social distancing measures were lifted on 18April 2022.
Literature Review: Novelty of this Study
This section provides a literature review and presents this study’s novelty. After the onset of the COVID-19 pandemic in 2019, various studies have been carried out. However, many studies have pursued research on viral tendencies rather than policy effects.
First, in this study, weekly data were used to analyze the relationship between the COVID-19 policies and the COVID-19 reproduction number in South Korea using RDD. Many previous studies predicted diffusion trends using simulation techniques (Balmford et al., 2020; Hsiang et al., 2020; Pei & Shaman, 2020; Wibbens et al., 2020, Kim, 2021; Kim et al., 2021).
Second, this study collected data from 17 metropolitan governments in South Korea for analysis. Although COVID-19 has affected the world, its impacts can be different depending on the characteristics of each country from an administrative and ecological viewpoint. Some studies have conducted a batch study covering a large number of countries (Chaudhry et al., 2020; Hsaing et al., 2020; Wibbens et al., 2020; Han & Park, 2021; Ko et al., 2021).
Lastly, this study used the reproduction number as a dependent variable and analyzed the effects on the infection reproduction index by classifying the COVID-19-related policies into business closure, private gathering limit, and vaccine pass requirement. Regarding domestic COVID-19 studies, research on the effects of emergency disaster relief funds had been conducted, focusing on some economic aspects (Lim, 2020; Lee & Hong, 2021; Nam & Lee, 2021), and research on household income and expenditure was also conducted (Hong & Ko, 2021).
Research Design, Methods, and Data
Regression Discontinuity Model
The regression discontinuity design (RDD), one of several quasi-experimental methods, was first introduced by Donald L. Thislethwaite and Donald T. Campbell in 1960. The RDD has been popularly used to measure the treatment effects of public policy. In this design, the assignment of control and treatment groups is determined by whether the assignment variable exceeds the cutoff point, or not. For example, when we are measuring the impact of government subsidy on low-income households who earns lower than USD1,000 per month, the monthly income would be the assignment variable, and households earning just below the cutoff point (USD1,000) would be the treatment group. By comparing the performance difference between treatment and control groups, the causal effect of government subsidy can be measured.
The RDD assumes that those just below the threshold of the assignment variable and those just above the threshold are approximately similar to each other. The only difference is the introduction of a treatment that allows a randomized experiment where the identification of a causal effect can be estimated (Thoemmes et al., 2017, p. 342). The basic idea of RDD is illustrated in Figure 1. If it is reasonable to assume that all factors are evolving smoothly with respect to the assignment variable, would be a reasonable guess for the value of of an individual scoring . Similarly, would be a reasonable guess for that same individual in the counterfactual state of not having the treatment. Then, could be viewed as an estimate of the causal effect of the treatment (Lee & Lemieux, 2010, p. 286).
Figure 1. A Simple Linear Regression Discontinuity Design
An article on BBC (March 12, 2020) titled “Coronavirus in Korea: How 'trace, test, and treat' may be saving lives” stated, “as the coronavirus spreads rapidly around the world, killing thousands and leaving governments scrambling to deal with the fallout, one country has repeatedly drawn praise for its efficiency in dealing with it: South Korea.” Since the first confirmed case of COVID-19 was reported on 20 January 2020, South Korea has been coping with the virus using a wide range of policy measures. The Korea Disease Control and Prevention Agency (KDCA), which was the headquarters of disease management, started the production of diagnostic test kits after a massive-scale outbreak on 18 February 2020 in Daegu City. As fatality and infection numbers grew, social distancing became one of the major policy measures adopted to prevent the spread of COVID-19 (Kim 2021). With the introduction of a five-tier alert system, social distancing restricted large-scale gatherings and outdoor activities of the public. High-risk facilities for contracting the virus—such as restaurants, coffee shops, pubs, clubs, PC rooms, karaoke, and indoor event halls—had to be closed before 9 p.m., and even entirely shut down depending on the level of social distancing. In January 2021, the KDCA further issued a restriction on private gatherings of more than four people, which was the first and the most rigorous restriction.
Meanwhile, the South Korean government adopted a digital-data-based management to geolocate COVID-19 patients and trace people who had been closely in contact with them. For instance, when patients are identified, South Korean local governments sent them a real-time text message that provided self-quarantine rules, and placed them under self-quarantine for two weeks. The local governments also traced the places where the patients had visited, using the record of credit card transactions and the Global Positioning System (GPS) data of the patients’ mobile phones (Kim 2021). By sharing the traced information to the public through the “emergency-alert-system announcement,” the local governments were able to further identify close contacts of the patients. In more recent years, the South Korean government introduced a “vaccine pass” system which helped the identification of vaccinated citizens by using a quick response (QR) code. A person who had received more than two times of COVID-19 vaccination was allowed to patronize densely populated facilities.
In response to the government efforts for coping with the pandemic, a growing body of study has focused on comparing different types of COVID-19 policies and drawing the trend line of infection. However, most studies have been concerned with predicting future trends of infection rather than examining the policy effects against the spread of COVID-19 (Balmford et al., 2020; Hsaing et al., 2020; Pei and Shaman, 2020; Wibbens et al., 2020, Kim, 2021; Kim et al., 2021). In addition, only a few research examined the effectiveness of COVID-19 policies in South Korea (Lim, 2020; Lee and Hong, 2021; Nam and Lee, 2021). Given the various types of restriction policies that have been introduced within a short period of time, further research efforts examining the policy effects of COVID-19 countermeasures are required.
In this regard, this study examines the effectiveness of COVID-19 policies in South Korea. By focusing on social distancing rules, it reveals the causal relationship between COVID-19 policies and the reproduction number of the disease. Using a sharp regression discontinuity design with a non-parametric estimation, it focuses on three specific types of restrictions and examines each policy effect on restraining the virus transmission: (1) business closure, (2) private gathering limit, and (3) vaccine pass requirement. In this study, the weekly data of infectees and casualties from 17 metropolitan governments in South Korea are used. This study is expected to increase the understanding of COVID-19 policies in South Korea and add empirical evidence in disease disaster management.
Background of the Study
Government Response to Transmission Dynamics
The first case of COVID-19 in South Korea was reported on 20 January 2020—a Chinese national who had recently traveled from the province of Hubei, People’s Republic of China. On 18 February, the first massive COVID-19 outbreak in the country (as of November 2020) began with the 31st case of COVID-19 identified in Daegu, the fourth most populous metropolitan city of South Korea and home to 2.2 million individuals. Close contacts of the 31st case were particularly clustered around a nationwide religious group known as Shincheonji. By 8 March 2020, 4,482 positive cases were identified from the religious group, comprising the majority of the total of 7,478 cases. From then on, there was a quick decline in the number of domestic infections, meaning that imported cases once again comprised the majority. Apart from the Daegu outbreak in March, there were two notable domestic outbreaks: one occasion linked to an Itaewon nightclub in Seoul on 2 May and a considerably larger outbreak on 15 August, linked to political protests in Gwanghwamun, Seoul. Although these two outbreaks did not result in a surge of cases as sharp as the Daegu outbreak, these were notable events in terms of their impact on subsequent intervention rollouts and public controversies around privacy and compliance.
The government took interventions in quick response to the transmission dynamics. One of the first notable changes was the border policy. A mandatory quarantine period of 14 days had been in place since 1 April 2020. Another notable intervention featuring the government’s responsiveness is seen in its testing capacity for COVID-19, specifically the timeline for increasing the testing capacity. Two responsive interventions—border control and extensive testing—proved effective in mitigating the influx of exogenous cases of COVID-19 into the country. After following domestic outbreaks, central and local governments set new policies called social distancing on 29 February 2020. A more relaxed measure was implemented on 6 May 2020 when there was a decreased infection trend. Since then, the government changed the alert levels according to daily infection rates, which also implied that varying social distancing measures would take place accordingly.
In South Korea, COVID-19 is considered a serious public health emergency, and the situation is being managed as a national disaster response case, triggering the disaster response governance mechanism. According to the manual, the infectious disease response system operates on different alert levels. At Level 1, countermeasure teams are organized at the KDCA. The Central Disease Control Headquarters at the KDCA is formed and operated at Level 2, while the Central Disaster Management Headquarters is formed and supports the Central Disease Control Headquarters at Level 3. At the highest level (Level 4), the participation of the Central Disaster and Safety Countermeasure Headquarters (CDSCH) is activated.
The central role of the CDSCH is to undertake policy dialogues and decision-making for major policies such as social distancing, inter-ministerial coordination, and facilitation of discussion between central and local governments. The organizational structure is as follows. At the center of the structure is the head (currently the Prime Minister), while the deputy head is the Minister of Interior and Safety. Under the CDSCH’s supervision are the Central Disease Control Headquarters and Central Disaster Management Headquarters, the National Fire Agency, and the Coast Guard, which can directly dispatch and undertake response missions, as well as other ministries and agencies. Each of the ministries and agencies sometimes operates local units and organizations directly, or through working relationship channels with local government counterparts. As the CDSCH is a non-standing body, a COVID-19 operation center was established under the Prime Minister’s office to support the Prime Minister’s role as the CDSCH head. This COVID-19 operation center prepares CDSCH meetings, coordinates between ministries, and communicates directly with the Office of National Security or with the President. The COVID-19 operation center is within the Prime Minister’s office and is subdivided into teams: the general affairs team, which takes care of CDSCH meetings and risk communication; the supporting team, which provides daily operational support to the prime minister; and the current issue management team, which deals with current issues such as vaccine rollouts, and maintains relationships with medical communities.
Social Distancing Level
During the first wave in February 2020, South Korea had yet to implement a well-defined social distancing scheme. As the first wave peaked in March 2020, the government enhanced its social distancing measures in April and May 2020. When the number of confirmed cases stayed at the lowest level, the government refined the social distancing scheme for the first time and spelled out the plans according to each level. The scheme played a key role during the second wave. During the government’s response, there was a greater need for a more detailed plan. When the level retreated to Level 1 in October 2020, the government further refined the scheme and published the second amendment. In this revised policy, there were five levels of social distancing measures with specific details regarding the scope of each level. One of the key changes was that the local government was given the authority to set the social distancing level. Not long after the amendment, the third wave began at the end of November 2020. As situations in the metropolitan area and some regions aggravated, both the central and local governments reacted by increasing the social distancing level.
Regarding school closures, the government faced several difficult decisions. When the first wave broke out in February 2020, a new academic year was about to begin, but every school was kept closed until March 2020. The Ministry of Education directed schools to open virtually in April 2020, and as the first wave subsided, the Ministry of Education let the schools partially open. Gradually, students were able to go to schools under strict infection control measures, including hand washing, indoor and outdoor mask-wearing, physical distancing, daily check for symptoms, and self-isolation for those with symptoms. Consequently, South Korea did not face serious incidences of school-based infections.
Among the 127 confirmed adolescent cases from 1 May to 12 July 2020, only three were attributed to public education and kindergartens. Most cases were instead family (59 cases) and private lesson-related (18 cases) incidences. In the second semester, starting in late August 2020, more students were expected to attend school. However, only one-third to two-thirds of students were allowed to attend school at a time, when the exact number or percentage of students was dependent on the level of social distancing. Many academics and experts in the country stressed the importance of a continuum of education and policy measures to minimize education disparity and prevent domestic violence.
Restrictions on facilities with high infection risks were a crucial part of social distancing. All facilities were asked to maintain logbooks for visitors, check symptoms and temperatures at entrances, place hand sanitizers, deliver proper instructions to visitors, and disinfect venues regularly. Moreover, facilities such as restaurants, coffee shops, pubs, clubs, karaoke, and indoor concert and event halls were designated as facilities with a high risk of transmission. These facilities had to close before 9 p.m. or shut down entirely, depending on the level of social distancing. Some raised concerns over these restrictions, in particular the economic costs of social distancing that were not equally imposed and left the self-employed vulnerable. In December 2020, the country further issued a ban on private gatherings of more than four people, deeming it the highest level of restriction barring complete lockdowns.
Recently, Omicron has become a major variant, compared with Delta, which was much more contagious. The Korean government, responding to this new wave, updated its policy to impose social distancing and adopted a new monitoring system using self-diagnosis kits starting in February 2021. Although many medical experts optimistically predicted that the final stage of the COVID-19 pandemic was at hand, all social distancing measures were lifted on 18April 2022.
Literature Review: Novelty of this Study
This section provides a literature review and presents this study’s novelty. After the onset of the COVID-19 pandemic in 2019, various studies have been carried out. However, many studies have pursued research on viral tendencies rather than policy effects.
First, in this study, weekly data were used to analyze the relationship between the COVID-19 policies and the COVID-19 reproduction number in South Korea using RDD. Many previous studies predicted diffusion trends using simulation techniques (Balmford et al., 2020; Hsiang et al., 2020; Pei & Shaman, 2020; Wibbens et al., 2020, Kim, 2021; Kim et al., 2021).
Second, this study collected data from 17 metropolitan governments in South Korea for analysis. Although COVID-19 has affected the world, its impacts can be different depending on the characteristics of each country from an administrative and ecological viewpoint. Some studies have conducted a batch study covering a large number of countries (Chaudhry et al., 2020; Hsaing et al., 2020; Wibbens et al., 2020; Han & Park, 2021; Ko et al., 2021).
Lastly, this study used the reproduction number as a dependent variable and analyzed the effects on the infection reproduction index by classifying the COVID-19-related policies into business closure, private gathering limit, and vaccine pass requirement. Regarding domestic COVID-19 studies, research on the effects of emergency disaster relief funds had been conducted, focusing on some economic aspects (Lim, 2020; Lee & Hong, 2021; Nam & Lee, 2021), and research on household income and expenditure was also conducted (Hong & Ko, 2021).
Research Design, Methods, and Data
Regression Discontinuity Model
The regression discontinuity design (RDD), one of several quasi-experimental methods, was first introduced by Donald L. Thislethwaite and Donald T. Campbell in 1960. The RDD has been popularly used to measure the treatment effects of public policy. In this design, the assignment of control and treatment groups is determined by whether the assignment variable exceeds the cutoff point, or not. For example, when we are measuring the impact of government subsidy on low-income households who earns lower than USD1,000 per month, the monthly income would be the assignment variable, and households earning just below the cutoff point (USD1,000) would be the treatment group. By comparing the performance difference between treatment and control groups, the causal effect of government subsidy can be measured.
The RDD assumes that those just below the threshold of the assignment variable and those just above the threshold are approximately similar to each other. The only difference is the introduction of a treatment that allows a randomized experiment where the identification of a causal effect can be estimated (Thoemmes et al., 2017, p. 342). The basic idea of RDD is illustrated in Figure 1. If it is reasonable to assume that all factors are evolving smoothly with respect to the assignment variable, would be a reasonable guess for the value of of an individual scoring . Similarly, would be a reasonable guess for that same individual in the counterfactual state of not having the treatment. Then, could be viewed as an estimate of the causal effect of the treatment (Lee & Lemieux, 2010, p. 286).
Figure 1. A Simple Linear Regression Discontinuity Design
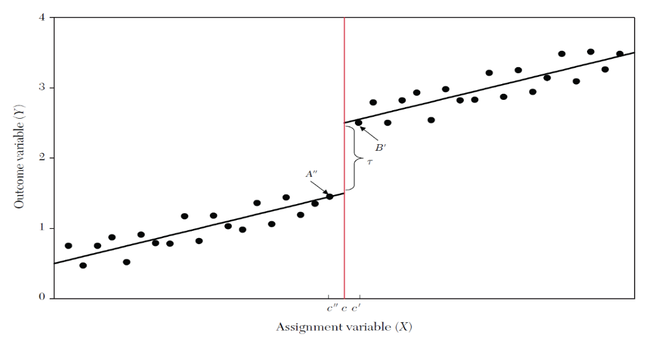
Source: Lee and Lemieux (2010, p. 286)
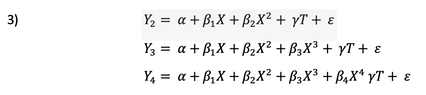
Two different types of methods have been used for estimation in the RDD: (1) parametric estimation and (2) non-parametric estimation. Parametric estimation is a global strategy that fits a statistical model to the data based on specific functional forms. In linear regression, it can be represented by the following simple equation:
Two different types of methods have been used for estimation in the RDD: (1) parametric estimation and (2) non-parametric estimation. Parametric estimation is a global strategy that fits a statistical model to the data based on specific functional forms. In linear regression, it can be represented by the following simple equation:

In this equation, denotes the assignment variable that causally affects the outcome variable . The treatment term, , denotes a dummy variable determined around the cutoff point, such that we have

The coefficient represents the causal effect of the treatment around the cutoff point. By estimating the parameter , RDD allows measuring the positive or negative impact of the treatment on the outcome variable. The estimation of the coefficient can differ from functional assumptions. For example, if we assume non-linear forms such as polynomial forms, they can be represented by different equations such as the following:
When it comes to parametric estimation, therefore, it is a significant challenge to select an appropriate discontinuous form. Substantial effort has been made to decide the fittest functional form, such as the F-test approach (Lee &Lemieux, 2010), the AIC approach (Bloom, 2009), and starting from an over-fitting model to a simple one by eliminating non-significant orders (Trochim, 1980). Despite of those approaches, parametric analysis is now often supplemented by non-parametric and semi-parametric estimation because of the poor approximation at around the cutoff point.
Non-parametric estimation is normally used to measure the local effect of the treatment around the cutoff point. This only considers points close to the threshold by employing different degrees of bandwidth. Using a linear or polynomial regression line, a non-parametric model usually considers a weighted regression, giving higher weights to individuals who are closer to the threshold. Therefore, it is important in this model to know how to choose the bandwidth that determines the weights (Thoemmes et al., 2017, p. 344).
The assignment variable is expected to be a single determinant causing the treatment . Therefore, all observed individuals ranging over the cutoff point are assumed to receive the treatment, meaning that the probability of the treatment jumps from 0 to 1 at the threshold. We call this a sharp RDD. However, in practice, the treatment could be determined partly by an assignment variable because of other factors that might affect the probability of individual participation or imperfect compliance. In this situation, the probability of the treatment does not switch from 0 to 1, but to other values ranging between 0 and 1. We refer to this as a fuzzy RDD.
Figure 2. Probability Change in a Sharp Regression Discontinuity Design and a Fuzzy Regression Discontinuity Design
Non-parametric estimation is normally used to measure the local effect of the treatment around the cutoff point. This only considers points close to the threshold by employing different degrees of bandwidth. Using a linear or polynomial regression line, a non-parametric model usually considers a weighted regression, giving higher weights to individuals who are closer to the threshold. Therefore, it is important in this model to know how to choose the bandwidth that determines the weights (Thoemmes et al., 2017, p. 344).
The assignment variable is expected to be a single determinant causing the treatment . Therefore, all observed individuals ranging over the cutoff point are assumed to receive the treatment, meaning that the probability of the treatment jumps from 0 to 1 at the threshold. We call this a sharp RDD. However, in practice, the treatment could be determined partly by an assignment variable because of other factors that might affect the probability of individual participation or imperfect compliance. In this situation, the probability of the treatment does not switch from 0 to 1, but to other values ranging between 0 and 1. We refer to this as a fuzzy RDD.
Figure 2. Probability Change in a Sharp Regression Discontinuity Design and a Fuzzy Regression Discontinuity Design
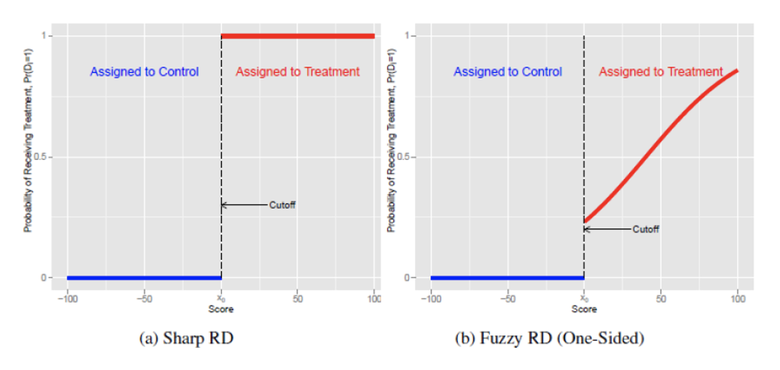
Source: Skovron and Titiunik (2015, p.5)
Empirical Model and Data
This study uses a sharp RDD with a non-parametric estimation to analyze the causal effects of different types of restriction policies to restrain COVID-19 transmission. The model uses the most popular data-driven bandwidth selection algorithm suggested by Imbens and Kalyanaraman (2009). Since early 2020, when the first confirmed case of COVID-19 occurred, the South Korean government has been implementing several restriction policies with regard to social distancing. These policies include business closure and curfew of facilities with high risk of infection, restriction on private gatherings exceeding a certain number of people, and a vaccine pass requirement that allows only people who have received several vaccine shots to patronize densely populated facilities. The study focused on three specific types of restriction: (1) business closure, (2) private gathering limit, and (3) vaccine pass requirement. The study measured each policy’s impact on restraining virus transmission.
Regarding the assignment variable and its cutoff point, the date of introduction of each policy is the clearest threshold in our model. In this regard, this study designs every single week as an assignment variable, which started from 19-25January 2020 and ends on 17-23 April 2022. The cutoff points are defined as each week of the introduction of the policies. Table 1 shows the research model with assignment, outcome, and treatment variables.
Table 1. Research Model
Empirical Model and Data
This study uses a sharp RDD with a non-parametric estimation to analyze the causal effects of different types of restriction policies to restrain COVID-19 transmission. The model uses the most popular data-driven bandwidth selection algorithm suggested by Imbens and Kalyanaraman (2009). Since early 2020, when the first confirmed case of COVID-19 occurred, the South Korean government has been implementing several restriction policies with regard to social distancing. These policies include business closure and curfew of facilities with high risk of infection, restriction on private gatherings exceeding a certain number of people, and a vaccine pass requirement that allows only people who have received several vaccine shots to patronize densely populated facilities. The study focused on three specific types of restriction: (1) business closure, (2) private gathering limit, and (3) vaccine pass requirement. The study measured each policy’s impact on restraining virus transmission.
Regarding the assignment variable and its cutoff point, the date of introduction of each policy is the clearest threshold in our model. In this regard, this study designs every single week as an assignment variable, which started from 19-25January 2020 and ends on 17-23 April 2022. The cutoff points are defined as each week of the introduction of the policies. Table 1 shows the research model with assignment, outcome, and treatment variables.
Table 1. Research Model
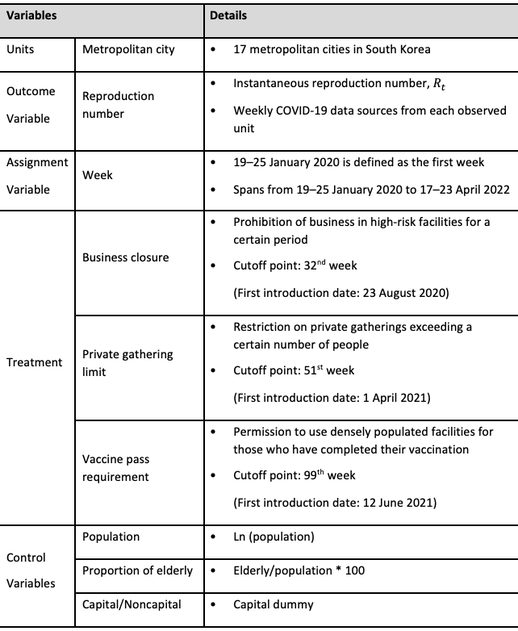
In disease management, such as the COVID-19 pandemic, quantifying the rate of transmissibility and controlling the number of cases are essential for governmental intervention. The reproduction number is a key epidemiological parameter that quantifies the average number of new infections caused by a single infected individual (O’Driscoll et al., 2021). By monitoring , governments get feedback on the effectiveness of their interventions and decide whether to intensify the control efforts to reduce below the threshold value of 1 and get as close as possible to 0, thus “bringing an epidemic under control” (Cori et al., 2013, p. 1505). When a pathogen emerges in an entirely susceptible population, the parameter is referred to as the basic reproduction number . It reflects the potential change of pathogen transmission without any external intervention, such that it can be mostly used at the early stage of infection. After the virus spreads and some population-level immunity has been achieved, this parameter is then referred to as the effective reproduction number . One of the effective reproduction numbers is the instantaneous reproduction number , which estimates the average number of secondary infections generated by infected individuals at the specific time of . It is most popularly used during an infectious period because it can be reported daily, or over a certain time window under the assumption that is constant within that period, which enables controlling an instant change in the pathogen’s transmissibility.
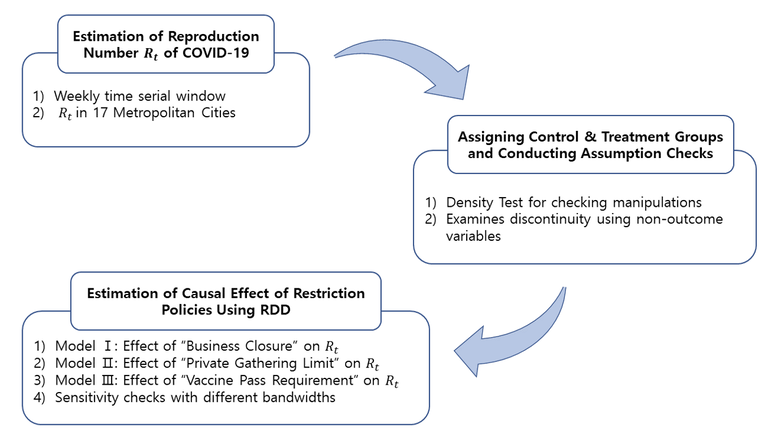
In this light, the study used the instantaneous reproduction number as an outcome variable, , which can differ as time passes. This study defines the time window size as seven days and uses the estimation method suggested by Cori et al. (2013) with a serial interval of 4.8 of the mean and 2.3 of the standard deviation. This study sets the prior mean of the reproduction number of COVID-19 as 3.7, such that can be estimated based on this parameter.[1]Figure 3 shows the flow of research.
Figure 3. Research Flow: Estimating the Causal Effect of the Restriction Policies
In this light, the study used the instantaneous reproduction number as an outcome variable, , which can differ as time passes. This study defines the time window size as seven days and uses the estimation method suggested by Cori et al. (2013) with a serial interval of 4.8 of the mean and 2.3 of the standard deviation. This study sets the prior mean of the reproduction number of COVID-19 as 3.7, such that can be estimated based on this parameter.[1]Figure 3 shows the flow of research.
Figure 3. Research Flow: Estimating the Causal Effect of the Restriction Policies
Major Findings
Descriptive Analysis
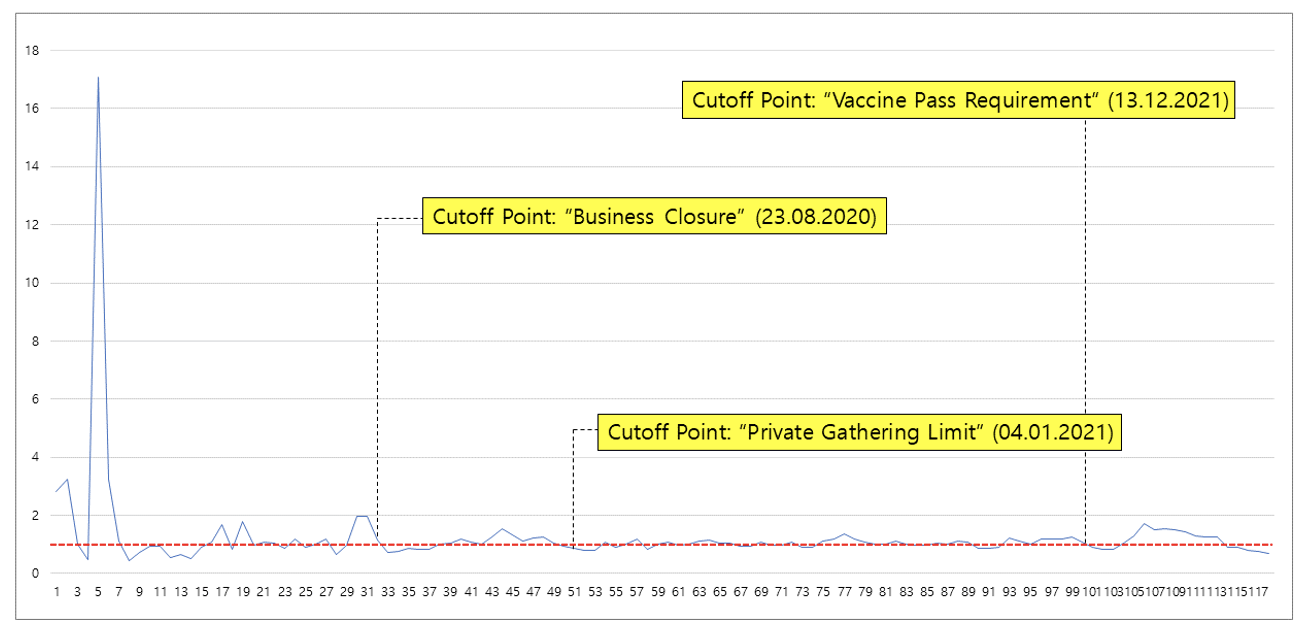
A graphical presentation of an RDD is helpful and informative, even though it does not provide any empirical evidence that proves whether there is a treatment effect. It has been standard practice to summarize the RDD analysis with a simple graph showing the relationship between the outcome and assignment variables (Lee &Lemieux, 2010). Figure 4 shows the changes in the weekly instantaneous reproduction number from 19–25 January 2020 (labeled as the 1st week) to 17–23 April 2022 (labeled as the 118th week). This was calculated from the merged data from 17 metropolitan cities to grasp the overall change in COVID-19’s transmissibility in South Korea. The horizontal dashed line indicates the threshold value . When , then the infection has spread among the population, which means that more than one person could be further infected by the pathogen. When , there is a lesser possibility for further infection, such that the pandemic is less likely to spread. In this study, , which started from 3.7, peaked during the 5th to 8th weeks and stayed at more than 1 point for most of the period, showing the high transmissibility of COVID-19. After introducing the first restriction policy, business closure, in the 32nd week, which suspended the business operations of highly infectious facilities such as bars, PC rooms, karaoke (singing room), and large academies, was temporarily going down to the threshold value of 1. The same phenomenon can be observed after the introduction of the second (51st week) and the third (100th week) restriction policies, which suggests that these policies might have resulted in the changes in .
Figure 4. Changes in the Weekly COVID-19 Reproduction Number in South Korea
Descriptive Analysis
A graphical presentation of an RDD is helpful and informative, even though it does not provide any empirical evidence that proves whether there is a treatment effect. It has been standard practice to summarize the RDD analysis with a simple graph showing the relationship between the outcome and assignment variables (Lee &Lemieux, 2010). Figure 4 shows the changes in the weekly instantaneous reproduction number from 19–25 January 2020 (labeled as the 1st week) to 17–23 April 2022 (labeled as the 118th week). This was calculated from the merged data from 17 metropolitan cities to grasp the overall change in COVID-19’s transmissibility in South Korea. The horizontal dashed line indicates the threshold value . When , then the infection has spread among the population, which means that more than one person could be further infected by the pathogen. When , there is a lesser possibility for further infection, such that the pandemic is less likely to spread. In this study, , which started from 3.7, peaked during the 5th to 8th weeks and stayed at more than 1 point for most of the period, showing the high transmissibility of COVID-19. After introducing the first restriction policy, business closure, in the 32nd week, which suspended the business operations of highly infectious facilities such as bars, PC rooms, karaoke (singing room), and large academies, was temporarily going down to the threshold value of 1. The same phenomenon can be observed after the introduction of the second (51st week) and the third (100th week) restriction policies, which suggests that these policies might have resulted in the changes in .
Figure 4. Changes in the Weekly COVID-19 Reproduction Number in South Korea
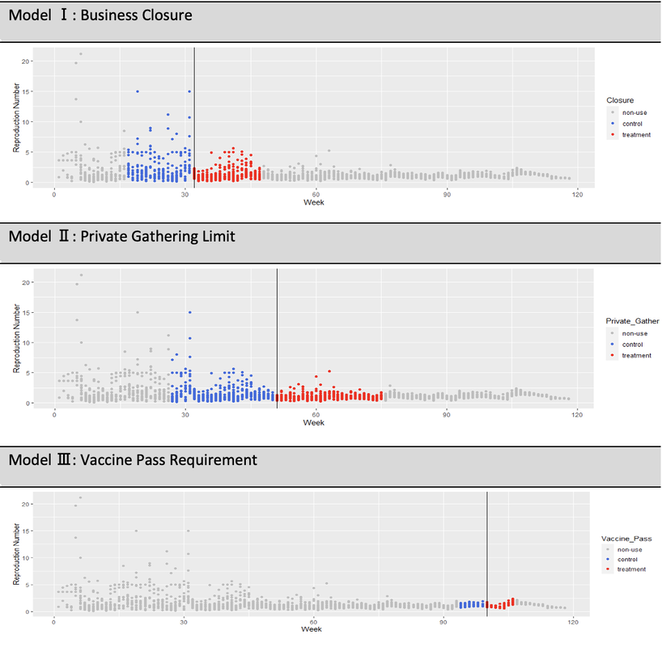
Even though it might be presumed that there was a positive policy effect on controlling the transmissibility of COVID-19, there is a need to analyze whether each restrictive policy did reduce the through an RDD. The scatter plots in Figure 5 provide more detailed information on the distinction between the control and treatment groups in each RDD analysis. Referring to the data-driven bandwidth selection process suggested by Imbens and Kalyanaraman (2009), this study used only the observed units close to each cutoff point to estimate the local average treatment effect (LATE). By setting the bandwidth, this study was able to get the coefficients without less bias in a non-parametric RDD. For example, in the first RDD analysis named model Ⅰ, 255 units represented by the blue dots were included in the control group. Meanwhile, 272 units represented by the red dots were used as the treatment group in the analysis. Similarly, there were 408 control units and 425 treatment units used in model Ⅱ, while 102 control units and 119 treatment units were used in model Ⅲ. Each vertical line refers to the cutoff point that indicates the introduction of the restriction policy.
Figure 5. Scatter Plots: Distinction between the Control and Treatment Groups
Figure 5. Scatter Plots: Distinction between the Control and Treatment Groups
One of the main assumptions under RDD is that individuals cannot precisely manipulate the assignment variable. This implies that the existence of a treatment being a discontinuous function of an assignment variable is not sufficient to justify the validity of an RDD (Lee & Lemieux, 2010). If individuals are unable to precisely manipulate the value of the assignment variable, the number of treated observations just above the threshold should be approximately similar to the number of control observations just below it. Therefore, checking the density of observations around the cutoff point is essential to support the validity of the RDD analysis results. However, in this study, this study used time (week) as an assignment variable, meaning that the observed individual cannot be available to manipulate the assignment variable. In other words, this study was able to observe the 17 metropolitan cities’ samples every single week, which made no graphical change in its density histogram (see Appendix 2). For this reason, this study can support the validity of the regression result without any further statistical tests.
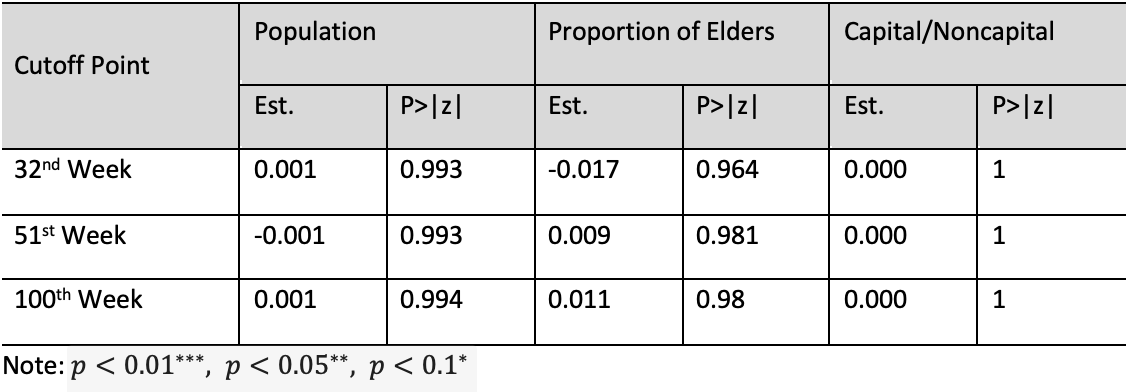
The other assumption under RDD is that all other factors that determine the outcome variable must be evolving smoothly. If the other variables also jump at the threshold, the gap between two discontinuous lines will potentially be biased for the treatment effect of interest (Lee & Lemieux, 2010). For this reason, this study conducted the same regression analysis using a non-outcome variable that might affect the change in as dependent variables. Table 2shows no discontinuity in the non-outcome variables, which supports the validity of the discontinuity design. In other words, there might be no other exogenous factors that cause discontinuity around each cutoff point. If any discontinuity occurs, it might be attributed to the treatment with a high possibility.
Table 2. Test of Discontinuity in Non-outcome Variables in the Regression Discontinuity Design
The other assumption under RDD is that all other factors that determine the outcome variable must be evolving smoothly. If the other variables also jump at the threshold, the gap between two discontinuous lines will potentially be biased for the treatment effect of interest (Lee & Lemieux, 2010). For this reason, this study conducted the same regression analysis using a non-outcome variable that might affect the change in as dependent variables. Table 2shows no discontinuity in the non-outcome variables, which supports the validity of the discontinuity design. In other words, there might be no other exogenous factors that cause discontinuity around each cutoff point. If any discontinuity occurs, it might be attributed to the treatment with a high possibility.
Table 2. Test of Discontinuity in Non-outcome Variables in the Regression Discontinuity Design
Empirical Results of RDD Analysis
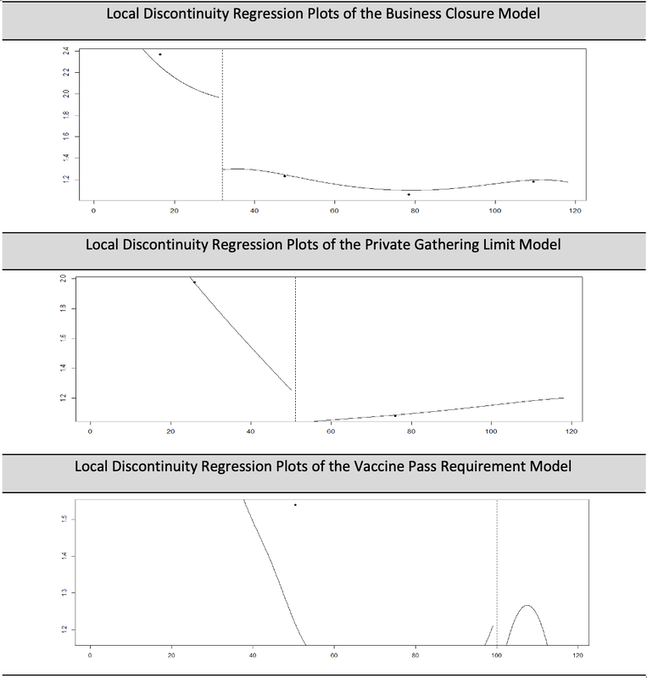
Table 3 shows the LATE of each restriction policy on the instantaneous reproduction number, in South Korea. If comes significantly down right after the introduction of the policy, it could be said that the policy has a positive effect on controlling COVID-19’s transmissibility. Looking closely at each cutoff point, the results show that the policies have a significant positive effect on decreasing in all three models. For the first model “business closure,” it turns out that dramatically decreased by 205% points after metropolitan city governments prohibited the business operations of high-risk facilities. This result implies that the spread of COVID-19 was significantly related to particular places such as bars, clubs, PC rooms, and karaoke. Moreover, this result suggests that the metropolitan governments effectively handled the transmissibility of COVID-19 by using a high level of restriction. The result is visualized clearly in Figure 6. Within the bandwidth size of 15.614, the regression plot of flows around 2.0 to 2.4 points and goes down to 1.3 points when it passes the cutoff point line in the 32nd week.
The same positive LATE is observed in the second model “private gathering limit,” even though the coefficient value is a little bit smaller than in the first model. This result implies that banning private gatherings of more than four people in densely populated facilities such as restaurants, cafés, and gyms had a positive effect on moderating the spread of COVID-19 (i.e., 28% points lower). Figure 6 shows the regression plot changes in around the second cutoff point, the 51st week. Compared with the business closure model, the gap between each separated regression line is much smaller around the threshold.
“Vaccine pass requirement,” which allowed those who had completely received COVID-19 vaccination to patronize densely populated facilities, helped control COVID-19’s transmissibility by decreasing by 35% points. Noting the highest level of local , this model shows that “vaccine pass” had a positive policy effect on controlling the spread of COVID-19. The result is depicted in Figure 6, which shows the discontinuity of the regression line within the bandwidth.
Table 3. Regression Results: Sharp RDD with a Non-parametric Estimation
Table 3 shows the LATE of each restriction policy on the instantaneous reproduction number, in South Korea. If comes significantly down right after the introduction of the policy, it could be said that the policy has a positive effect on controlling COVID-19’s transmissibility. Looking closely at each cutoff point, the results show that the policies have a significant positive effect on decreasing in all three models. For the first model “business closure,” it turns out that dramatically decreased by 205% points after metropolitan city governments prohibited the business operations of high-risk facilities. This result implies that the spread of COVID-19 was significantly related to particular places such as bars, clubs, PC rooms, and karaoke. Moreover, this result suggests that the metropolitan governments effectively handled the transmissibility of COVID-19 by using a high level of restriction. The result is visualized clearly in Figure 6. Within the bandwidth size of 15.614, the regression plot of flows around 2.0 to 2.4 points and goes down to 1.3 points when it passes the cutoff point line in the 32nd week.
The same positive LATE is observed in the second model “private gathering limit,” even though the coefficient value is a little bit smaller than in the first model. This result implies that banning private gatherings of more than four people in densely populated facilities such as restaurants, cafés, and gyms had a positive effect on moderating the spread of COVID-19 (i.e., 28% points lower). Figure 6 shows the regression plot changes in around the second cutoff point, the 51st week. Compared with the business closure model, the gap between each separated regression line is much smaller around the threshold.
“Vaccine pass requirement,” which allowed those who had completely received COVID-19 vaccination to patronize densely populated facilities, helped control COVID-19’s transmissibility by decreasing by 35% points. Noting the highest level of local , this model shows that “vaccine pass” had a positive policy effect on controlling the spread of COVID-19. The result is depicted in Figure 6, which shows the discontinuity of the regression line within the bandwidth.
Table 3. Regression Results: Sharp RDD with a Non-parametric Estimation
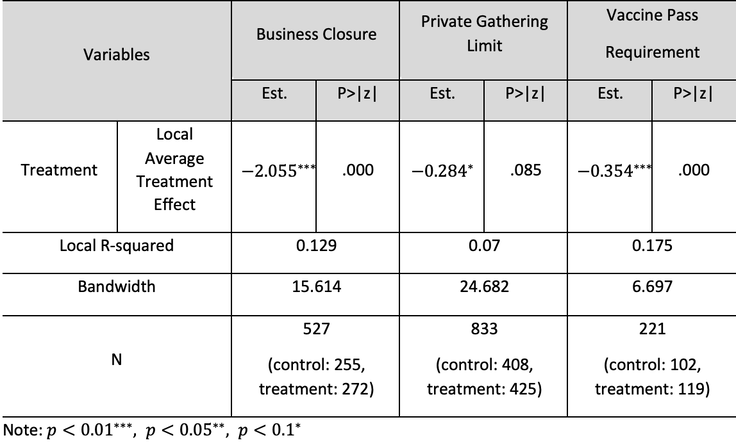
Figure 6. Local Discontinuity Regression Plots of the Models
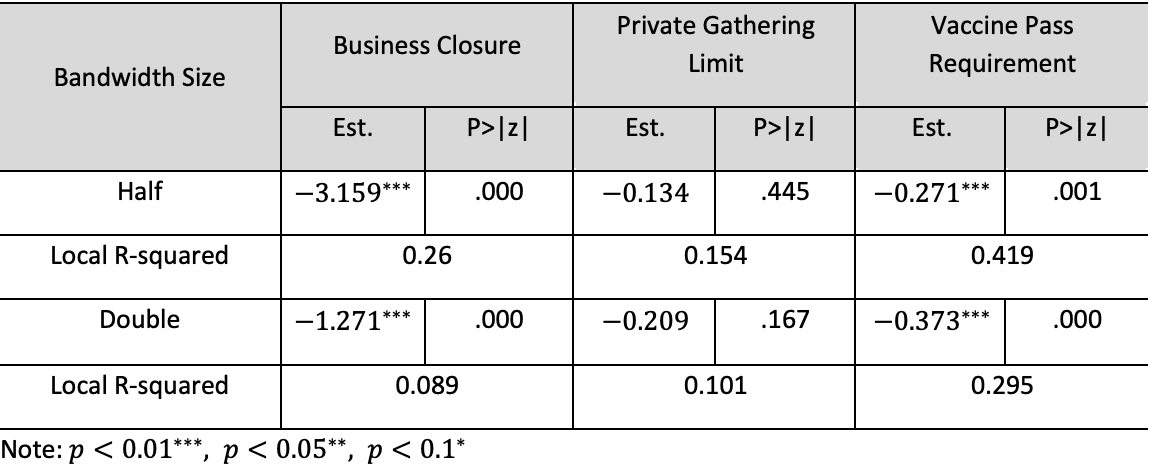
This study conducted a sensitivity check that employed a half and a double bandwidth size from the original one. The choice of bandwidth for the local approach is critical because different choices yield different estimates of the treatment effect. Ideally, the treatment effect remains stable across various bandwidth choices. Table 4 presents the results of the sensitivity test, which shows that the effect remains relatively constant for most choices of bandwidth. With a narrowing bandwidth, a negative LATE is still observed in models Ⅰ and Ⅲ without losing its significance. In addition, the estimates remain stable in the widened bandwidth choice, partially owing to the increased sample size. However, for model Ⅱ, the significant treatment effect was not observed in both the narrow and wide bandwidths. This is an indication that the results of model Ⅱ from the original regression are less credible than those of the other models. Therefore, caution must be exercised when accepting that restricting the private gathering limit had a positive policy effect on restraining virus transmission.
Table 4. Sensitivity Test Using Different Bandwidth Sizes
Table 4. Sensitivity Test Using Different Bandwidth Sizes
Findings and Discussion
This section provides a summary of the RDD analysis results and the related validity tests. First, the restriction policies implemented by the South Korean government during the COVID-19 pandemic had a positive effect on decreasing the transmissibility of the virus. Specifically, the first restrictive policy “business closure,” which suspended the business operations of high-risk facilities, showed a strong controlling effect on the transmissibility of COVID-19. There is a reduction of the value of by 205% points, which was the biggest reduction of among the three different restrictive policies. Private gathering limit and vaccine pass requirement showed the corresponding policy effects by decreasing to 28% and 35% points for each, which were both significant to be accepted.
The empirical results demonstrate that the traditional strategy of completely blocking out the possibility of contact among people by closing high-risk facilities and banning large gatherings could be a reliable strategy during pandemics. This is partially supported by the evidence that “business closure” and “private gathering limit” had a positive effect on decreasing in this study. A novel finding of this study is that the digital capacity of the government could play a significant role in disease disaster management. In practice, the “vaccine pass requirement” was highly reliant upon the digital capacity of central and local governments. Specifically, it required updated records ofindividuals who had received COVID-19 vaccination and traced them through spatial data reported via a mobile application. Without this digital capacity, it would be difficult to distinguish between individuals who had and had not completed their vaccination, making it challenging to introduce such a restrictive policy.
Therefore, for future disease disaster management, not only the traditional approach but also the digital approach must be considered as an alternative management strategy. The traditional approach indeed has a credible policy result, but it is also true that closing down facilities and banning private gatherings lead to economic losses, as all economic activities are shut down. As the digital approach enables the introduction of a selective restriction policy, thisapproach might be a way to minimize economic losses while controlling the spread of the disease.
Conclusion: Lesson and Recommendations
Since its first outbreak in 2019, the COVID-19 pandemic has been one of the most devastating global disasters, resulting in millions of casualties worldwide. While governments have exerted tremendous efforts to control and eradicate the virus, the unprecedented nature of COVID-19 calls into question whether a traditional government system has successfully contributed in terms of rapid public delivery, local governance, and digital capacities. This study analyzed the effectiveness of South Korea’s COVID-19 policy by focusing on the causal relationship between COVID-19’s reproduction number and the restriction policies of “business closure,” “private gathering limit,” and “vaccine pass requirement.” Using a sharp RDD with a non-parametric estimation, the study found a positive effect of each restriction policy on decreasing COVID-19 transmission. Although these results should be understood in the context of South Korea, there might be a meaningful implication to countries that have implemented or plan to introduce similar restrictive policies for disaster management.
This study’s findings have critical implications because it highlights the effective and smart ICT infrastructure and transparent big data tracing system of South Korea, which were an excellent digital foundation for its success. On 27–28 October 2021, the Indonesian Association for Public Administration held its annual international forum to examine the developments in public administration. The theme “Governance and Public Policy in Society 5.0” was adopted in response to the increasing need for knowledge and skills in the current era. One definition of Society 5.0 is a human-centered society that balances economic advancement with people’s quality of life. A huge amount of information from sensors in the physical space is accumulated in cyberspace, with the results—analyzed using artificial intelligence and big data—expected to enhance the well-being of human life.
Recently, Harvard University’s John F. Kennedy School of Government established a new policy research center named Future Society. Echoing J. F. Kennedy’s famous vision, “on the edge of a new frontier,” and from the perception of new technologies in the fourth industrial revolution, the research think tank embarked on new research about “nano, bio, information, cognitive” (NBIC) brain science and new creative policy initiatives. They emphasized the need for a new vision of effective policymaking under the circumstances of a turbulent society, as our society is facing an array of crucial ethical questions and policy choices.
We are facing a new and different turn and a more chaotic and turbulent society, characterized by volatility, uncertainty, complexity, and ambiguity. We are not only witnessing new developments in technology but also facing a global pandemic that is greatly changing our social life. Such revolutionary challenges require a clear-eyed evaluation of existing governance models and operating systems. Industry 4.0, artificial intelligence (AI), NBIC, a new global health crisis, and other social and natural disasters are ahead of us, posing heightened uncertainty. We must seriously consider a new agile governance model with a greater digital capacity based on an integrative approach. Super smart technologies such as the internet-of-things (a meta-verse formed by fusing cyberspace and physical space), big data, and AI are facilitating a new agile governance model and making a new agile governance model more feasible, as discussed earlier regarding Korea’s COVID-19 policies. What does this Korean experience with policy strategy as a pandemic response tell other Asian countries? No doubt, each country has different historical trajectories, and there is no single best solution or panacea. The best solution for one country, oftentimes, does not work for another. Nevertheless, one thing is clear: digital government with agile and responsible leadership has become crucial.
This section provides a summary of the RDD analysis results and the related validity tests. First, the restriction policies implemented by the South Korean government during the COVID-19 pandemic had a positive effect on decreasing the transmissibility of the virus. Specifically, the first restrictive policy “business closure,” which suspended the business operations of high-risk facilities, showed a strong controlling effect on the transmissibility of COVID-19. There is a reduction of the value of by 205% points, which was the biggest reduction of among the three different restrictive policies. Private gathering limit and vaccine pass requirement showed the corresponding policy effects by decreasing to 28% and 35% points for each, which were both significant to be accepted.
The empirical results demonstrate that the traditional strategy of completely blocking out the possibility of contact among people by closing high-risk facilities and banning large gatherings could be a reliable strategy during pandemics. This is partially supported by the evidence that “business closure” and “private gathering limit” had a positive effect on decreasing in this study. A novel finding of this study is that the digital capacity of the government could play a significant role in disease disaster management. In practice, the “vaccine pass requirement” was highly reliant upon the digital capacity of central and local governments. Specifically, it required updated records ofindividuals who had received COVID-19 vaccination and traced them through spatial data reported via a mobile application. Without this digital capacity, it would be difficult to distinguish between individuals who had and had not completed their vaccination, making it challenging to introduce such a restrictive policy.
Therefore, for future disease disaster management, not only the traditional approach but also the digital approach must be considered as an alternative management strategy. The traditional approach indeed has a credible policy result, but it is also true that closing down facilities and banning private gatherings lead to economic losses, as all economic activities are shut down. As the digital approach enables the introduction of a selective restriction policy, thisapproach might be a way to minimize economic losses while controlling the spread of the disease.
Conclusion: Lesson and Recommendations
Since its first outbreak in 2019, the COVID-19 pandemic has been one of the most devastating global disasters, resulting in millions of casualties worldwide. While governments have exerted tremendous efforts to control and eradicate the virus, the unprecedented nature of COVID-19 calls into question whether a traditional government system has successfully contributed in terms of rapid public delivery, local governance, and digital capacities. This study analyzed the effectiveness of South Korea’s COVID-19 policy by focusing on the causal relationship between COVID-19’s reproduction number and the restriction policies of “business closure,” “private gathering limit,” and “vaccine pass requirement.” Using a sharp RDD with a non-parametric estimation, the study found a positive effect of each restriction policy on decreasing COVID-19 transmission. Although these results should be understood in the context of South Korea, there might be a meaningful implication to countries that have implemented or plan to introduce similar restrictive policies for disaster management.
This study’s findings have critical implications because it highlights the effective and smart ICT infrastructure and transparent big data tracing system of South Korea, which were an excellent digital foundation for its success. On 27–28 October 2021, the Indonesian Association for Public Administration held its annual international forum to examine the developments in public administration. The theme “Governance and Public Policy in Society 5.0” was adopted in response to the increasing need for knowledge and skills in the current era. One definition of Society 5.0 is a human-centered society that balances economic advancement with people’s quality of life. A huge amount of information from sensors in the physical space is accumulated in cyberspace, with the results—analyzed using artificial intelligence and big data—expected to enhance the well-being of human life.
Recently, Harvard University’s John F. Kennedy School of Government established a new policy research center named Future Society. Echoing J. F. Kennedy’s famous vision, “on the edge of a new frontier,” and from the perception of new technologies in the fourth industrial revolution, the research think tank embarked on new research about “nano, bio, information, cognitive” (NBIC) brain science and new creative policy initiatives. They emphasized the need for a new vision of effective policymaking under the circumstances of a turbulent society, as our society is facing an array of crucial ethical questions and policy choices.
We are facing a new and different turn and a more chaotic and turbulent society, characterized by volatility, uncertainty, complexity, and ambiguity. We are not only witnessing new developments in technology but also facing a global pandemic that is greatly changing our social life. Such revolutionary challenges require a clear-eyed evaluation of existing governance models and operating systems. Industry 4.0, artificial intelligence (AI), NBIC, a new global health crisis, and other social and natural disasters are ahead of us, posing heightened uncertainty. We must seriously consider a new agile governance model with a greater digital capacity based on an integrative approach. Super smart technologies such as the internet-of-things (a meta-verse formed by fusing cyberspace and physical space), big data, and AI are facilitating a new agile governance model and making a new agile governance model more feasible, as discussed earlier regarding Korea’s COVID-19 policies. What does this Korean experience with policy strategy as a pandemic response tell other Asian countries? No doubt, each country has different historical trajectories, and there is no single best solution or panacea. The best solution for one country, oftentimes, does not work for another. Nevertheless, one thing is clear: digital government with agile and responsible leadership has become crucial.
References
Balmford, B., Annan, J. D., Hargreaves, J. C., Altoè, M., & Bateman, I. J. (2020). Cross-country comparisons of Covid-19: policy, politics and the price of life. Environmental and Resource Economics, 76, 525-551.
Bicker L. (2020). Coronavirus in South Korea: How 'trace, test and treat' may be saving lives. BBC News. https://www.bbc.com/news/world-asia-51836898
Bloom, N. (2009). The impact of uncertainty shocks. Econometrica, 77(3), 623-685.
Chaudhry, R., Dranitsaris, G., Mubashir, T., Bartoszko, J., & Riazi, S. (2020). A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes. EClinicalMedicine, 25, 100464. https://doi.org/10.1016/j.eclinm.2020.100464
Cori, A., Ferguson, N. M., Fraser, C., & Cauchemez, S. (2013). A new framework and software to estimate time-varying reproduction numbers during epidemics. American journal of epidemiology,178(9), 1505-1512.
Han C. Y., & Park S. A. (2021). The effect of the containment and closure policies on the spread of COVID-19. The Korean Association for Policy Studies, 30(3), 1-38.
Hong. M. J., & Ko K. K. (2021). Universal health coverage and effectiveness of response to COVID-19: Focusing on out-of-pocket health expenditure. Korean Public Administration Review, 55(3), 125-153.
Hsiang, S., Allen, D., Annan-Phan, S., Bell, K., Bolliger, I., Chong, T., ... & Wu, T. (2020). The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature, 584(7820), 262-267.
Imbens, G., & Kalyanaraman, K. (2009). Optimal bandwidth choice for the regression discontinuity estimator (Working Paper No. 14726).National Bureau of Economic Research. doi,10, w14726.
Kim D., Chung Y., & Lee, K. (2021). An analysis of the effects of a segmented social distancing policy in response to COVID-19. Journal of Korean System Dynamics Society, 22(1), 37-57.
Kim, P. S. (2021). South Korea’s fast response to coronavirus disease: implications on public policy and public management theory. Public Management Review, 23(12), 1736-1747.
Kim. S. G. (2021). Estimating the effects of social distancing for COVID-19: Applying spatially explicit SEPIR model. The Korean Association for Policy Studies, 30(3), 237-270.
Ko, K., Huh, J., & Park, J. (2021). Comparative study of the trend and policy: Response of COVID-19 in global cities. Journal of local government studies, 33(2), 93-118.
Laura Bicker. (2020.03.12). Coronavirus in South Korea: How 'trace, test and treat' may be saving lives. BBC News, Seoul.
Lee S. H., & Hong. M. K. (2021). The effects of COVID-19 and emergency disaster relief funds on household income and expenditure in Korea. Korea Social Policy Review, 28(3), 17-44.
Lee, D. S., & Lemieux, T. (2010). Regression discontinuity designs in economics. Journal of economic literature,48(2), 281-355.
Lim T. K. (2020). Effectiveness of direct subsidies responses to COVID-19 on the job growth of small businesses in South Korea: Focused on quasi-experimental design. The Korean Journal of Local Government Studies, 24(3), 27-46.
Nam, J., & Lee, R. H. (2021). The influence of COVID-19 economic impact payment on household consumption in South Korea: Focusing on comparison by income classes. Social Welfare Policy, 48(1), 63-95.
O’Driscoll, M., Harry, C., Donnelly, C. A., Cori, A., & Dorigatti, I. (2021). A comparative analysis of statistical methods to estimate the reproduction number in emerging epidemics, with implications for the current coronavirus disease 2019 (COVID-19) pandemic. Clinical Infectious Diseases,73(1), e215-e223.
Pei, S., & Shaman, J. (2020). Initial simulation of SARS-CoV2 spread and intervention effects in the continental US. MedRxiv, 2020-03.
Pei, S., Kandula, S., & Shaman, J. (2020). Differential effects of intervention timing on COVID-19 spread in the United States. Science advances, 6(49), eabd6370.
Skovron, C., & Titiunik, R. (2015). A practical guide to regression discontinuity designs in political science. American Journal of Political Science, 2015, 1-36.
Thistlethwaite, D. L., & Campbell, D. T. (1960). Regression-discontinuity analysis: An alternative to the ex post facto experiment, Journal of Educational Psychology, 51(6), 309.
Thoemmes, F., Liao, W., & Jin, Z. (2017). The analysis of the regression-discontinuity design in R. Journal of Educational and Behavioral Statistics, 42(3), 341-360.
Trochim, W. M. K. (1980). The regression-discontinuity design in Title I evaluation: Implementation, analysis and variations. Northwestern University.
Wibbens, P. D., Koo, W. W. Y., & McGahan, A. M. (2020). Which COVID policies are most effective? A Bayesian analysis of COVID-19 by jurisdiction. PloS one, 15(12), e0244177.
Balmford, B., Annan, J. D., Hargreaves, J. C., Altoè, M., & Bateman, I. J. (2020). Cross-country comparisons of Covid-19: policy, politics and the price of life. Environmental and Resource Economics, 76, 525-551.
Bicker L. (2020). Coronavirus in South Korea: How 'trace, test and treat' may be saving lives. BBC News. https://www.bbc.com/news/world-asia-51836898
Bloom, N. (2009). The impact of uncertainty shocks. Econometrica, 77(3), 623-685.
Chaudhry, R., Dranitsaris, G., Mubashir, T., Bartoszko, J., & Riazi, S. (2020). A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes. EClinicalMedicine, 25, 100464. https://doi.org/10.1016/j.eclinm.2020.100464
Cori, A., Ferguson, N. M., Fraser, C., & Cauchemez, S. (2013). A new framework and software to estimate time-varying reproduction numbers during epidemics. American journal of epidemiology,178(9), 1505-1512.
Han C. Y., & Park S. A. (2021). The effect of the containment and closure policies on the spread of COVID-19. The Korean Association for Policy Studies, 30(3), 1-38.
Hong. M. J., & Ko K. K. (2021). Universal health coverage and effectiveness of response to COVID-19: Focusing on out-of-pocket health expenditure. Korean Public Administration Review, 55(3), 125-153.
Hsiang, S., Allen, D., Annan-Phan, S., Bell, K., Bolliger, I., Chong, T., ... & Wu, T. (2020). The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature, 584(7820), 262-267.
Imbens, G., & Kalyanaraman, K. (2009). Optimal bandwidth choice for the regression discontinuity estimator (Working Paper No. 14726).National Bureau of Economic Research. doi,10, w14726.
Kim D., Chung Y., & Lee, K. (2021). An analysis of the effects of a segmented social distancing policy in response to COVID-19. Journal of Korean System Dynamics Society, 22(1), 37-57.
Kim, P. S. (2021). South Korea’s fast response to coronavirus disease: implications on public policy and public management theory. Public Management Review, 23(12), 1736-1747.
Kim. S. G. (2021). Estimating the effects of social distancing for COVID-19: Applying spatially explicit SEPIR model. The Korean Association for Policy Studies, 30(3), 237-270.
Ko, K., Huh, J., & Park, J. (2021). Comparative study of the trend and policy: Response of COVID-19 in global cities. Journal of local government studies, 33(2), 93-118.
Laura Bicker. (2020.03.12). Coronavirus in South Korea: How 'trace, test and treat' may be saving lives. BBC News, Seoul.
Lee S. H., & Hong. M. K. (2021). The effects of COVID-19 and emergency disaster relief funds on household income and expenditure in Korea. Korea Social Policy Review, 28(3), 17-44.
Lee, D. S., & Lemieux, T. (2010). Regression discontinuity designs in economics. Journal of economic literature,48(2), 281-355.
Lim T. K. (2020). Effectiveness of direct subsidies responses to COVID-19 on the job growth of small businesses in South Korea: Focused on quasi-experimental design. The Korean Journal of Local Government Studies, 24(3), 27-46.
Nam, J., & Lee, R. H. (2021). The influence of COVID-19 economic impact payment on household consumption in South Korea: Focusing on comparison by income classes. Social Welfare Policy, 48(1), 63-95.
O’Driscoll, M., Harry, C., Donnelly, C. A., Cori, A., & Dorigatti, I. (2021). A comparative analysis of statistical methods to estimate the reproduction number in emerging epidemics, with implications for the current coronavirus disease 2019 (COVID-19) pandemic. Clinical Infectious Diseases,73(1), e215-e223.
Pei, S., & Shaman, J. (2020). Initial simulation of SARS-CoV2 spread and intervention effects in the continental US. MedRxiv, 2020-03.
Pei, S., Kandula, S., & Shaman, J. (2020). Differential effects of intervention timing on COVID-19 spread in the United States. Science advances, 6(49), eabd6370.
Skovron, C., & Titiunik, R. (2015). A practical guide to regression discontinuity designs in political science. American Journal of Political Science, 2015, 1-36.
Thistlethwaite, D. L., & Campbell, D. T. (1960). Regression-discontinuity analysis: An alternative to the ex post facto experiment, Journal of Educational Psychology, 51(6), 309.
Thoemmes, F., Liao, W., & Jin, Z. (2017). The analysis of the regression-discontinuity design in R. Journal of Educational and Behavioral Statistics, 42(3), 341-360.
Trochim, W. M. K. (1980). The regression-discontinuity design in Title I evaluation: Implementation, analysis and variations. Northwestern University.
Wibbens, P. D., Koo, W. W. Y., & McGahan, A. M. (2020). Which COVID policies are most effective? A Bayesian analysis of COVID-19 by jurisdiction. PloS one, 15(12), e0244177.
Appendix
Appendix 1. Descriptive Analysis Results
Appendix 1. Descriptive Analysis Results
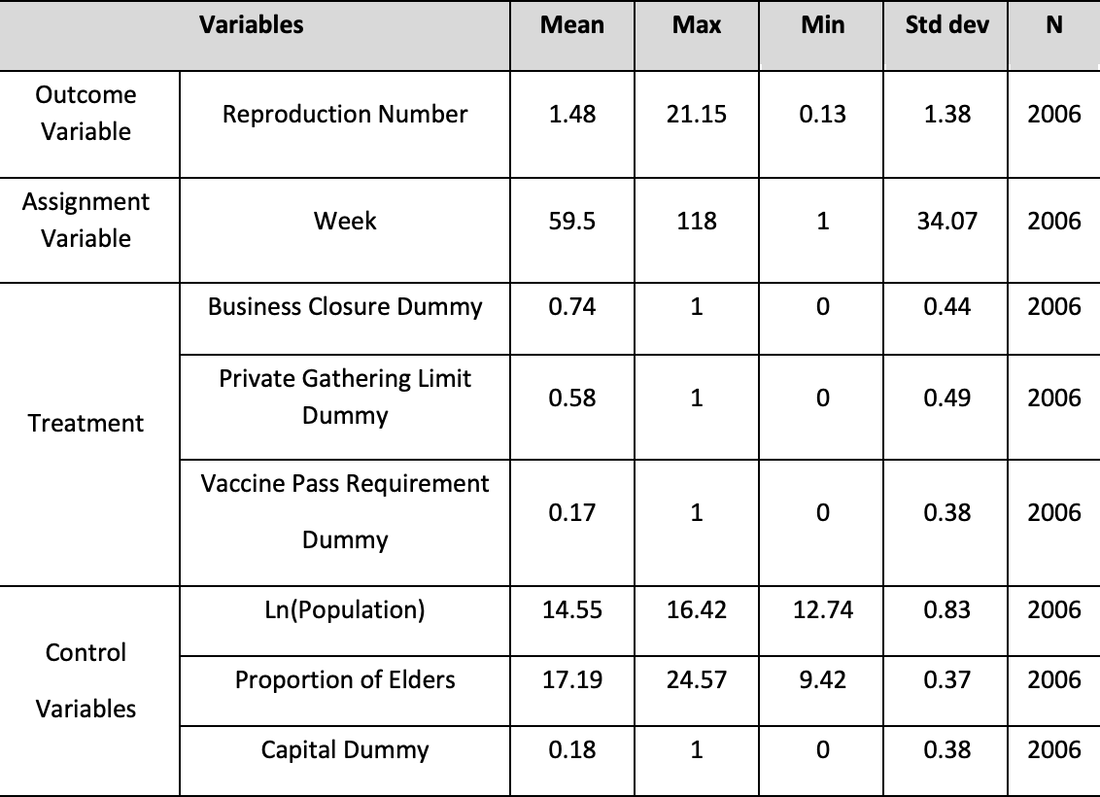
Appendix 2. Histogram of the Assignment Variable